People who have experienced trauma
Jump to a section below
Key considerations
People with intellectual disability experience high rates of trauma
Trauma is an emotional, physiological and cognitive response to a distressing event or series of events, such as acts of violence, natural disasters, interpersonal violence and accidents. Some people may have emotional or physical reactions that are severe and last a long time. People with intellectual disability experience high rates of traumatic and adverse life events, particularly violence and abuse. [1, 2] These experiences can lead to trauma-related disorders, including post-traumatic stress disorder (PTSD), which people with intellectual disability are thought to be more susceptible to developing. [3]
While most research studies agree that there is a high prevalence of trauma among people with intellectual disability, there is no standardised measure of trauma for this population. Most studies focus on childhood and adult abuse, bullying, and neglect, which will be our focus here also.
Life events may affect individuals differently
It is important to consider that a person’s experience of an event may be traumatic for them, even though it may not be traumatic for another individual. People with intellectual disability can experience many adverse life events and situations, such as:
- institutional care during childhood (even if no abuse occurred in care)
- frequent rejection
- loss of placements or primary carers at school, home and support services
- being in environments that they are unable to cope with (e.g. due to over-sensitivity)
- frequent health care visits.
In response, a person with intellectual disability may present with symptoms similar to those that might present after events more commonly associated with causing trauma.
Distressing or painful experiences while receiving health care in the past (where the person may not have understood what was happening) can lead people to resist seeking health care, including mental health care. This can have lifelong consequences.
Disability Royal Commission
The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (or Disability Royal Commission) has now ended. The Commission found that people with disability, including people with intellectual disability, have experienced violence, abuse, neglect and exploitation in health, education and learning, homes and living, relationships, justice settings and economic participation. View the Final report (including Easy Read versions) for all the findings and recommendations.
Key challenges in meeting the mental health needs of people with intellectual disability who have experienced trauma
Although people with intellectual disability experience high rates of trauma, past trauma is often not identified or considered when mental health care is provided. This may be due to communication difficulties, making it hard for people with intellectual disability to disclose past or current trauma. Behaviours of concern that occur as a result of trauma may also be wrongly attributed to the person’s intellectual disability, which can impede professionals’ ability to recognise or consider trauma when providing services.
Abuse, bullying or neglect may be a current experience for the person with intellectual disability. If not already appropriately supported to manage this experience, this may present a barrier to addressing their mental health needs. This is often because the person has not yet disclosed the abuse, bullying or neglect. There are various reasons why the person may not have disclosed this, including:
- communication difficulties
- sense of self or self-esteem difficulties
- limited or minimal safe relationships
- having a poor understanding of abuse, bullying and neglect
- fear of not being believed or of getting into trouble when disclosing (including a history of not being believed or listened to)
- not wanting the perpetrator to get into trouble (this may include being groomed by the perpetrator)
- prior experience of seeing poor outcomes for other people with intellectual disability who have reported abuse.
In some cases, the person may have disclosed the abuse but remains in the environment where the abuse is continuing (e.g. living in group accommodation with other residents who are aggressive, with no alternate placement option). This can also lead to barriers to addressing the person’s mental health needs.
People with intellectual disability may have less control over their lives and environment, which can make it difficult to avoid reminders or triggers related to past trauma. This can exacerbate mental health problems or cause added stress for the individual.
Triggers to previous trauma can often exist as thoughts, memories or physiological sensations. Physiological sensations can be anything related to your senses, including specific smells or being touched on a specific part of your body. Physiological sensations can emerge in relation to other activities or experience, thus triggering vivid memories of previous traumatic experiences with similar physiological sensations.
Mental health needs relating to trauma can be acute and/or chronic and impacting daily functioning. Specific mental health treatment needs are delivered by public and private mental health services, while psychosocial disability needs (as a result of trauma and associated mental health problems) related to daily functioning can be met by the NDIS. Systemic issues and lack of clarity by professionals around responsibility can result in people’s needs not being met by any system or service.
How I can meet the mental health needs of people with intellectual disability who have experienced trauma
What I should know
Abuse, bullying and neglect may all contribute to mental health problems or trauma that the person may be experiencing. Similar to people without intellectual disability, people with intellectual disability who have experienced abuse, bullying or neglect can display PTSD symptoms, poor self-esteem, nightmares, fear of sex following sexual abuse and feelings of self-harm and suicide. Depending on the person’s circumstances and living situation, when a person with intellectual disability presents with changes in behaviour or mental health, GPs and mental health professionals should consider the possibility of abuse, bullying or neglect as a contributing factor.
The basic principles of trauma-informed practice and support apply equally to a person with intellectual disability as they do for anyone else. You can read more about trauma-informed practice here.
What I should do
- Recognise that the person you support may have experienced adverse life events and the ongoing impacts of these.
- Work from a trauma-informed perspective. You will not always know what has happened to the person, even if you ask.
- Find out whether the person with intellectual disability is currently experiencing or has experienced adverse life events or abuse in the past. Provide capacity building support to the person, as relevant to your role, about their rights and options for support. You can use resources like Scope Australia’s Speak Up and Be Safe From Abuse resources toolkit, which was developed for people with communication difficulties to identify and report abuse.
- Be aware that, in some cases, abuse is not recognised as abuse by the person experiencing it. For example, it may have been normalised within the context of their lived experience.
What I should know
All service providers need to remain aware that there is a risk of abuse and neglect. If you suspect that something is wrong, you should take action.
What I should do
- Record any changes to the person or any signs that cause concern.
- Find out who else is already supporting the person with their trauma and mental health. Develop a collaborative plan, with appropriate consent, for providing integrated support for the person.
- Work with others who provide support and share any concerns with them so that signs of abuse can be recognised early.
- Depending on the person’s circumstances and living situation, when a person with intellectual disability presents with changes in behaviour or mental health, mental health professionals should consider the possibility of abuse or neglect as a contributing factor.
What I should know
Regardless of when the event(s) happened, if a person with intellectual disability discloses abuse or neglect to you, you should take action to ensure the immediate safety of the person. You can take action by following the steps below. Keep in mind that it is not your job to investigate what has happened – that is the job of the police. Your responsibility is to support the mental health and wellbeing of the person with intellectual disability.
What I should do
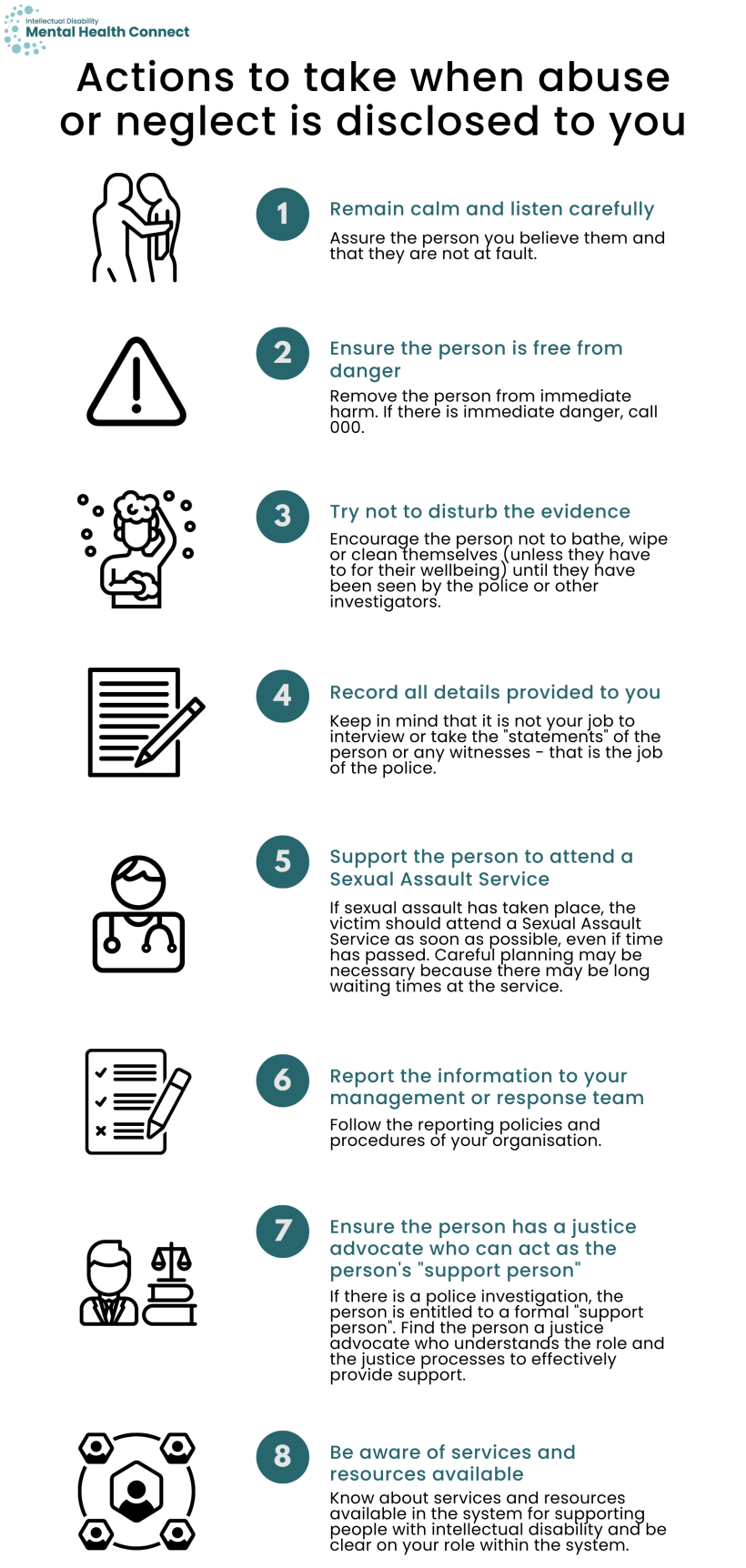
- Remain calm and listen carefully. You should assure the person that you believe them and that they are not at fault.
- Ensure that the person is free from danger by removing them from immediate harm and ensuring there is no further contact with the perpetrator. If there is immediate danger, call 000.
- Try not to disturb any evidence. Encourage the person not to bathe, wipe or clean themselves (unless they have to for their wellbeing) until they have been seen by police or other investigators.
- Record all details provided to you by the person with intellectual disability, using their exact words if possible. Keep in mind, however, that it is not your job to interview or take the “statements” of the person or any witnesses – that is the job of the police.
- If sexual assault has taken place, the victim should attend a Sexual Assault Service as soon as possible, even if time has passed. For a person with intellectual disability, careful planning may be necessary because there may be long waiting times at the service. You may also need to prepare the person for what might happen at the service. To find a Sexual Assault Service in NSW, see this page.
- Report the information to your management or response team as soon as possible, following the policies and procedures of your organisation.
- If there is a police investigation, people with intellectual disability are considered “vulnerable persons” in police regulations. This means that they are entitled to a formal “support person” during the investigation. It is important to get the person in touch with a justice advocate who can act as the “support person”, to ensure that the person’s rights are upheld. You can also act as a support person yourself though it is important that you have had appropriate training and understand the role and the justice processes to effectively provide this support. To find a justice advocate, you can contact the NSW Justice Advocacy Service. For additional information on how to support a person during police investigations, you may find our information on supporting a person in contact with the criminal justice system helpful.
- Be aware of services and resources available in the system for supporting people with intellectual disability, mental health and trauma histories, and be clear on your role within this.
What I should know
All service providers should be aware of their responsibilities as a mandatory reporter. Mandatory reporters are required by law to report suspected child abuse and neglect. Child abuse in any form is a criminal offence and should be reported immediately to FACS. If you are not sure if you are a mandatory reporter, you can check the list here.
Any criminal acts against both children and adults need to be reported to NSW Police. Criminal acts include physical abuse, sexual assault, some forms of financial abuse and any incident where the victim has suffered serious harm.
Registered NDIS providers must notify the NDIS Quality and Safeguards Commission of all reportable incidents that occur (or are alleged to have occurred) in connection with the provision of NDIS supports or services you deliver using the My Reportable Incidents page on the NDIS Commission Portal. Reportable incidents include:
- death of a person with disability
- serious injury of a person with disability
- abuse or neglect of a person with disability
- unlawful sexual or physical contact with, or assault of, a person with disability
- sexual misconduct, committed against, or in the presence of, a person with disability
- use of a restrictive practice in relation to a person with disability where the use is not in accordance with an authorisation.
The NDIS Commission must be notified within certain timeframes depending on the incident that has occurred. For more information about these timeframes and reportable incidents, see this page.
What I should do
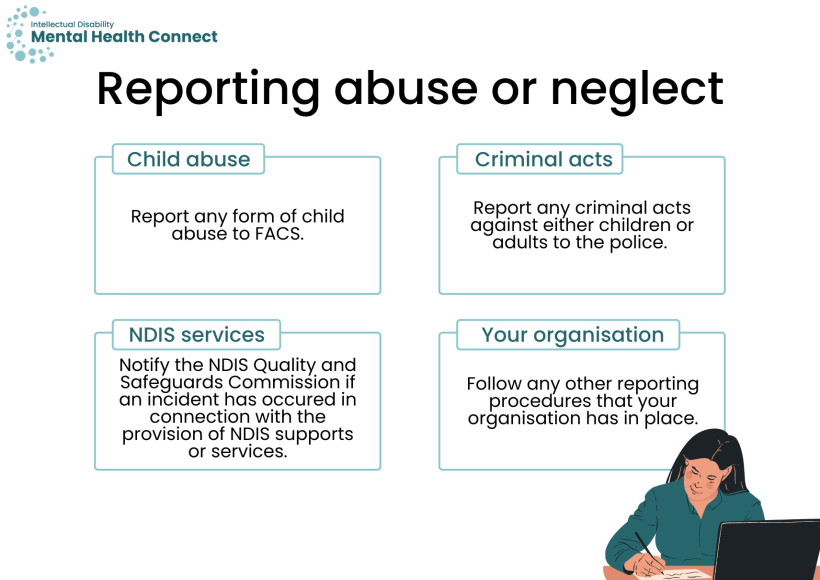
- Report any form of child abuse immediately to FACS.
- Report any criminal acts against either children or adults to NSW Police. Before doing so, develop a clear, informed plan about how this will be communicated to the person (and their guardian, if relevant), especially if the person is an adult and has capacity to make decisions about pursuing legal charges.
- If an incident has occurred in connection with the provision of NDIS supports or services, notify the NDIS Quality and Safeguards Commission. You can find more information about how to notify the NDIS Commission here.
- Follow any other reporting procedures that your organisation has in place.
What I should know
Bullying can be an issue in supported living and group homes, work and school. The bullying may be from other residents at the group home, colleagues or managers at work, or other students or staff at school. Like abuse and neglect, bullying can have a negative impact on the person with intellectual disability’s mental health and it is important to respond immediately if bullying is disclosed to you.
For more information about the experiences of people with intellectual disability living in group homes, see the documents from the Disability Royal Commission’s Public Hearing 3.
What I should do
- Encourage the person to keep a diary or you could help record information for them. It is important to document everything that has happened and all actions that have been taken to stop the bullying.
- Provide support to the person or help them get in touch with trusted people or support services such as:
- Kids Help Line (1800 55 1800), a free telephone counselling service for those aged 5-25 years
- Lifeline (13 11 14)
- a mental health professional.
- If the person has experienced any form of violence, assault or stalking, report this directly to NSW Police. These types of bullying are criminal offences.
- Ensure the person’s legal guardian, if applicable, is informed of any formal processes or other information as requested by them.
- Encourage or help the person with intellectual disability to tell someone, report the bullying or make a complaint.
- If the person with intellectual disability is experiencing bullying in supported living or their group home, support the person to report the bullying by speaking to a supervisor or manager at the home. If a staff member is bullying the person with intellectual disability, the home or organisation should have a procedure or policy in place to deal with this. Homes and organisations should ensure that their reporting processes are accessible and transparent. If another resident is bullying or disturbing a person in group home accommodation, disability support workers need to put a plan in place to manage this, as it can significantly affect the mental health of the person. Any accommodation changes for the person may require formal decision-making by an appointed guardian.
- If the person with intellectual disability is experiencing bullying at work, support the person to report the bullying by using the workplace reporting procedures first, or speaking to someone at the workplace, such as a supervisor or manager. You can also help the person to make a complaint to the Australian Human Rights Commission on 1300 656 419. SafeWork NSW can also provide advice on workplace bullying and can be contacted on 13 10 50.
- If a young person with intellectual disability is experiencing bullying at school, you can ask the school about their anti-bullying plan so that you can report the bullying. If appropriate action is not taken, you can support the person to escalate the complaint to the Department of Education and Training (if the person attends a public school).
More information about trauma-informed care and how to provide trauma-informed care to people with intellectual disability can be found in the guiding principles.
Key resources
- Disability Abuse and Neglect Hotline is a free and confidential service for reporting abuse and neglect of people with disability. They can be contacted at 1800 880 052 or [email protected]. The Hotline is not a crisis service.
- National Counselling and Support Service (1800 RESPECT) is a confidential counselling and support service that operates 24/7. They provide support to people who have experienced or are experiencing sexual assault, domestic or family violence and abuse.
- NSW Ageing and Disability Abuse Hotline aims to prevent older people and adults with disability from abuse, neglect and exploitation. The Hotline can be contacted at 1800 628 221.
- Victims Services provides counselling, financial assistance for immediate needs or economic loss and recognition payment to victims of violent crime in NSW. They can be contacted on 1800 633 063.
- Scope Australia’s Speak Up and Be Safe From Abuse is a resources toolkit developed for people with communication difficulties to identify and report abuse.
- FACS has information about mandatory reporters on this page.
- The NDIS Commission has information on what is a reportable incident and within what timeframe incidents need to be reported.
- The NDIS Commission has information on how to report an incident to the Commission.
- A list of NSW Sexual Assault Services can be found on this page.
- NSW Health has information about prevention and response to violence, abuse and neglect, including information about domestic and family violence, sexual assault, child protection and wellbeing, First Nations peoples’ family wellbeing and violence protection and children and young people with problematic or harmful sexual behaviours.
- NSW Health’s Integrated Prevention and Response to Violence, Abuse and Neglect Framework provides information about NSW Health’s response to violence, abuse and neglect, including available resources and services.
- The Australian Human Rights Commission has a factsheet about workplace bullying.
Additional background information
Abuse occurs when someone’s human rights are violated by the actions of another person. There are different forms of abuse. Some common forms that people with intellectual disability may experience and indicative signs are listed below. However, it is important to be mindful that these signs could indicate issues other than abuse (e.g. mental health problems).
| Types of abuse | Physical signs | Potential indirect signs |
|---|---|---|
| Physical abuse: when a person uses physical force against another person. Physical abuse can start off slowly and inconspicuously before getting more intense and frequent over time. |
|
|
| Emotional/psychological abuse: when a person maintains power and control by taking away another person’s confidence, independence or self-esteem. Verbal abuse is a key feature of emotionally abusive relationships. Verbal abuse is when a person consistently makes statements that negatively label another person. | Due to the nature of emotional abuse, you are more likely to see indirect signs than physical signs. |
|
| Sexual abuse: when a person commits any form of forced or unwanted sexual activity on or towards another person. |
|
|
| Social abuse: when a person prevents another person from spending time with family and friends and participating in social activities. | Due to the nature of social abuse, you are more likely to see indirect signs than physical signs. |
|
| Financial abuse: when a person manipulates another person’s financial decisions and controls their access to money or property without consent. |
|
|
| Institutional/systemic abuse: the maltreatment of a person from a system of power. Institutional or systemic abuse can occur within care facilities like residential facilities for people with intellectual disability, or health care services like inpatient settings. |
|
|
| Chemical abuse: withholding of prescribed medication or over-administration of medication in order to control behaviour. |
|
Abuse is not limited to just one form and anybody can experience it from anyone in any location.
Neglect is when a person intentionally or negligently fails to take care of another person physically, emotionally or financially, in breach of duty of care. Some examples of neglect include:
- the person being left alone for long periods of time when the risk of foreseeable harm or injury to the person requiring care would be high
- inadequate provision of, or support to access nutrition, clothing or personal hygiene
- failure to provide a safe environment
- failure to provide appropriate health care or medical treatment.
Bullying is when a person repeatedly and intentionally uses words or actions against another person or group of people to cause distress and risk to their wellbeing. It is not the same as disliking someone or having conflict with someone, though bullying might occur because of these reasons. We tend to think of bullying as something that happens in schools, but bullying can happen in any location (e.g. in group homes or at work) and can take different forms.
For more information on bullying, see this factsheet by the Australian Human Rights Commission.
The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability (or Disability Royal Commission) has now ended. The Final report has been released (including Easy Read versions). The key issues highlighted by the Disability Royal Commission included:
- Health:
- Systemic neglect of people with cognitive disability in the Australia health system
- Barriers to accessing health care, including:
- staff reluctance to provide appropriate care
- diagnostic overshadowing
- staff not listening to patients with disability
- Lack of education and training in working with people with cognitive disability, including in communication and facilitating decision-making
- Education and learning:
- Lack of access to education and the quality of education is not equitable for people with disability
- Some students with disability may be segregated
- Physical, verbal and emotional violence or abuse happens in educational settings, including inappropriate use of restrictive practices
- Additional key drivers and forms of violence, abuse and neglect in educational settings can be found on p.23 of the Interim Report Summary
- Homes and living:
- People with disability subjected to violence, abuse and neglect in private homes, group homes and supported accommodation
- Lack of choice around accommodation can also lead people to be exposed to abuse
- Casualisation of staff, poor training of support workers and punitive culture among staff were the other key themes
- Relationships:
- Higher rates of domestic and family violence and sexual violence experienced by people with disability
- Many experienced multiple forms of violence and abuse
- The COVID-19 pandemic meant increased isolation and reduced access to support networks and reduced opportunities to report abuse
- Economic participation:
- Experiences of violence and abuse in open and segregated employment, including physical, sexual and verbal abuse by colleagues and managers
- When issues of abuse have been raised, they have often been ignored or not appropriately addressed
- Justice:
- People with disability are not believed by police when reporting violence and abuse, and have often been treated as the offender rather than the complainant
- People with cognitive disability are at greater risk of violence, abuse and neglect in closed environments, with restrictive practices and solitary confinement used to manage them
- People with cognitive or psychosocial disability are disproportionately subjected to indefinite detention orders, which can mean that they are held longer than if they had been convicted
- Guardianship and administrative orders can limit the person’s choice and control, and may lead to violence, abuse and neglect, especially financial exploitation
- Mason-Roberts S, Bradley A, Karatzias T, Brown M, Paterson D, Walley R, et al. Multiple traumatisation and subsequent psychopathology in people with intellectual disabilities and DSM-5 PTSD: a preliminary study. Journal of Intellectual Disability Research. 2018;62(8): 730-6.
- Wigham S and Emerson E. Trauma and life events in adults with intellectual disability. Current Developmental Disorders Reports. 2015;2(2): 93-9.
- Byrne G. A Systematic Review of Treatment Interventions for Individuals With Intellectual Disability and Trauma Symptoms: A Review of the Recent Literature. Trauma, Violence, & Abuse. 2022;23(2): 541-54.